Fill Out Your Arizona Religious Beliefs Form
The Arizona Religious Beliefs form serves a crucial role in the intersection of public health and individual rights. This official document, mandated by Arizona law, is required for preschools and child care facilities when parents or guardians seek an exemption from immunization based on their religious beliefs. The Arizona Department of Health Services (ADHS) emphasizes the importance of vaccinations as a primary means of preventing serious diseases. However, it also acknowledges the rights of parents who adhere to religious teachings that oppose immunization. By completing this form, parents can formally exempt their child from specific vaccines, such as Diphtheria, Tetanus, Pertussis, and others, by marking an "X" next to the relevant diseases. Each section requires parents to acknowledge the potential risks associated with forgoing these vaccinations, which include severe health complications and even death. Furthermore, the form informs parents that they have the right to rescind the exemption at any time should they choose to vaccinate their child in the future. It is also important for parents to be aware that during an outbreak of a vaccine-preventable disease, unvaccinated children may be prohibited from attending child care facilities until the outbreak risk subsides. This form thus represents a delicate balance between respecting individual beliefs and safeguarding public health.
Guide to Writing Arizona Religious Beliefs
Completing the Arizona Religious Beliefs form is an important step for parents seeking an exemption from immunization based on their religious beliefs. The following steps will guide you through the process of filling out this form accurately.
- Obtain a copy of the Arizona Religious Beliefs Exemption Form from the Arizona Department of Health Services website or your local child care facility.
- Fill in your child's name and date of birth at the top of the form.
- Review the list of vaccines and their associated diseases. Place an “X” in the box next to each vaccine you wish to exempt your child from.
- For each vaccine you selected, initial in the space provided to indicate that you have been informed about the risks associated with not vaccinating your child.
- Next to each initial, write the date you completed that section.
- At the bottom of the form, acknowledge your request for an exemption by initialing the statement regarding your religious beliefs.
- Sign the form where indicated, and include the date of your signature.
Once you have completed the form, submit it to your child’s preschool or child care facility as required. Keep a copy for your records, and remember that you can change your mind about the exemption in the future if you choose to vaccinate your child.
Browse Popular Forms
Arizona Jt-1 - Community-specific tax rules may affect how you fill out the application.
How Much Does It Cost to File for Custody - The objections must be filed with the court within 14 days of receiving the subpoena.
Does Arizona Have Income Tax - Employees working in Arizona but residing out of state may need to consider their tax obligations.
Common Questions
What is the purpose of the Arizona Religious Beliefs form?
The Arizona Religious Beliefs form is designed for parents or guardians who wish to exempt their child from required vaccinations due to their religious beliefs. Arizona law mandates that preschools and child care facilities use this official form to document such exemptions. By completing this form, parents acknowledge their right to make vaccination decisions based on their religious convictions while also being informed about the potential health risks associated with not vaccinating their child.
How do I fill out the Arizona Religious Beliefs form?
To complete the form, you will need to place an “X” in the box next to each vaccine you are opting out of. After marking your choices, you must initial and date the corresponding box to confirm your understanding of the risks involved with not vaccinating. Additionally, provide your child’s name, date of birth, and your signature at the bottom of the form. This ensures that all necessary information is documented clearly and accurately.
What are the potential risks of not vaccinating my child?
Choosing not to vaccinate can expose your child to various serious diseases. Each vaccine protects against specific illnesses that can lead to severe health complications, including paralysis, brain damage, and even death. For example, not vaccinating against measles could result in pneumonia or brain damage, while skipping the polio vaccine could lead to paralysis. The form provides detailed information about the risks associated with each disease, helping you make an informed decision.
Can I change my mind after submitting the form?
Yes, you can change your mind. If you decide to rescind the exemption in the future, you can obtain the necessary immunizations for your child. It’s important to keep in mind that if there is an outbreak of a vaccine-preventable disease and your child does not have proof of immunity, they may not be allowed to attend child care until the risk period has ended, which can last several weeks.
Where can I find more information about vaccines and immunization services?
Additional information about vaccine-preventable diseases, vaccines, and low-cost vaccination services is available through your local county health department or the Arizona Department of Health Services. Their website, www.azdhs.gov/phs/immun/, is a valuable resource for parents seeking guidance on immunization and health services in Arizona.
Dos and Don'ts
When filling out the Arizona Religious Beliefs form, it is essential to follow specific guidelines to ensure that the process goes smoothly. Here are five things you should do and five things you should avoid.
- Do read the instructions carefully. Understanding the requirements will help you fill out the form correctly.
- Do provide accurate information. Ensure that all details, including your child's name and date of birth, are correct.
- Do initial and date each section. This shows that you acknowledge the information provided regarding the risks associated with not vaccinating.
- Do keep a copy of the completed form. Having a record can be helpful for future reference.
- Do contact your local health department if you have questions. They can provide assistance and additional information.
- Don't leave any sections blank. Incomplete forms may be rejected or delayed.
- Don't provide false information. Misrepresentation can lead to serious consequences.
- Don't forget to sign the form. An unsigned form is not valid.
- Don't ignore the potential consequences. Be aware that your child may not be allowed to attend child care during an outbreak.
- Don't hesitate to rescind the exemption if you change your mind. You have the right to change your decision regarding vaccinations.
Similar forms
The Arizona Medical Exemption Form is similar to the Religious Beliefs Exemption Form in that both documents allow parents to opt out of required vaccinations for their children. While the Religious Beliefs Exemption is based on the family's religious convictions, the Medical Exemption Form requires a healthcare provider’s signature, indicating that a medical condition prevents the child from receiving specific vaccines. This form serves as a safeguard for children who have legitimate health concerns, ensuring they are not put at risk from immunizations that could exacerbate their medical issues.
The Vaccine Exemption Form used in California also bears similarities to the Arizona Religious Beliefs form. Like its Arizona counterpart, this form allows parents to declare their child exempt from vaccinations due to personal beliefs. However, California has more stringent requirements, including a mandatory educational component for parents before they can submit the exemption. This ensures that parents are fully informed about the implications of opting out of vaccinations, which is a critical aspect of public health and safety.
The Personal Beliefs Exemption Form in Washington State provides another comparable document. It allows parents to exempt their children from vaccinations based on personal beliefs, including religious convictions. The key distinction here is that Washington requires parents to submit this form annually, reinforcing the commitment to informed decision-making regarding vaccinations. This annual renewal process serves to remind parents of the ongoing importance of vaccinations and the potential risks associated with non-vaccination.
The Immunization Exemption Request Form in New York shares a similar function, allowing parents to request exemptions from vaccination requirements for their children. New York's form, however, is more focused on the legal and procedural aspects, requiring a detailed explanation of the grounds for the exemption. This additional requirement emphasizes the need for parents to articulate their beliefs clearly, which can help health officials assess the legitimacy of the exemption request more thoroughly.
Lastly, the Religious Exemption Form in Texas is another document that parallels the Arizona Religious Beliefs Exemption. This form allows parents to cite their religious beliefs as a reason for not vaccinating their children. However, Texas law also mandates that parents submit a notarized affidavit, which adds an extra layer of verification to the exemption process. This requirement helps ensure that the exemption is not only a matter of personal belief but is also formally recognized, thereby maintaining the integrity of the vaccination system while respecting individual rights.
Key takeaways
Official Requirement: Arizona law mandates the use of the Arizona Religious Beliefs form for documenting a religious exemption to immunizations in preschools and child care facilities.
Informed Consent: Parents must acknowledge the potential health risks associated with not vaccinating their child by initialing and dating each vaccine listed on the form.
Understanding Risks: The form details serious health consequences for each vaccine-preventable disease, emphasizing the importance of informed decision-making.
Right to Rescind: Parents can rescind the exemption at any time and choose to vaccinate their child in the future.
Outbreak Protocol: In the event of an outbreak, unvaccinated children may be barred from attending child care until the risk period concludes, which could last for three weeks or longer.
Common mistakes
-
Not placing an “X” in the box next to the disease(s) selected. This is crucial for indicating which vaccines you are exempting your child from.
-
Failing to initial next to each disease. Initials confirm that you understand the risks associated with not vaccinating.
-
Neglecting to provide the date next to each initial. Dates are important for tracking when the exemption was requested.
-
Overlooking the section where you must sign as the parent or guardian. This signature is a legal acknowledgment of your request.
-
Not including your child's full name and date of birth. This information is essential for properly identifying your child.
-
Ignoring the information about potential consequences during an outbreak. Understanding these implications is important for making informed decisions.
-
Submitting the form without reviewing it for completeness. Double-checking can prevent delays or issues with the exemption.
-
Failing to keep a copy of the submitted form. Retaining a copy is important for your records and future reference.
Document Preview
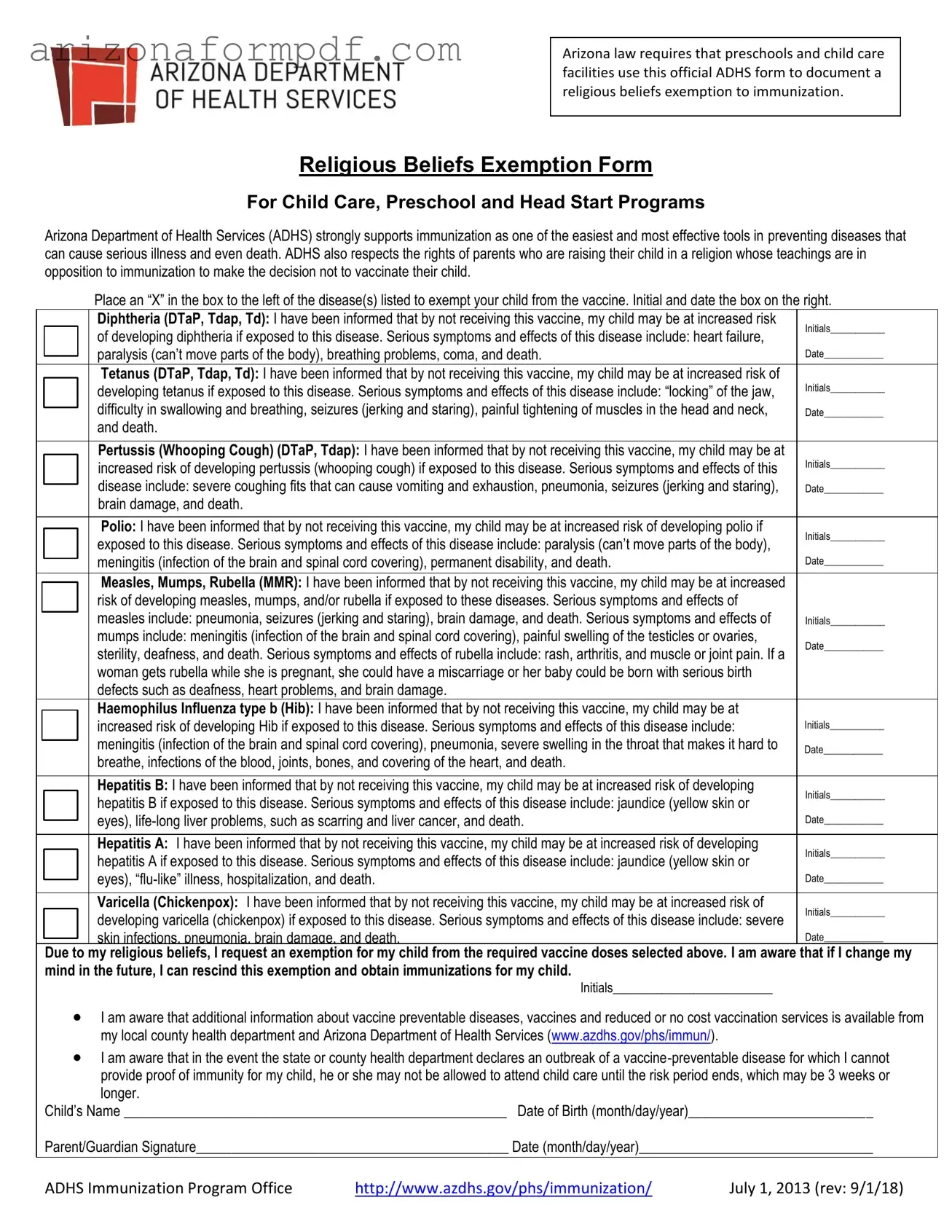
Arizona law requires that preschools and child care facilities use this official ADHS form to document a religious beliefs exemption to immunization.
Religious Beliefs Exemption Form
For Child Care, Preschool and Head Start Programs
Arizona Department of Health Services (ADHS) strongly supports immunization as one of the easiest and most effective tools in preventing diseases that can cause serious illness and even death. ADHS also respects the rights of parents who are raising their child in a religion whose teachings are in opposition to immunization to make the decision not to vaccinate their child.
Place an “X” in the box to the left of the disease(s) listed to exempt your child from the vaccine. Initial and date the box on the right.
|
|
|
Diphtheria (DTaP, Tdap, Td): I have been informed that by not receiving this vaccine, my child may be at increased risk |
Initials___________ |
|
|
|
of developing diphtheria if exposed to this disease. Serious symptoms and effects of this disease include: heart failure, |
|
|
|
|
|
|
|
|
|
paralysis (can’t move parts of the body), breathing problems, coma, and death. |
Date____________ |
|
|
|
||
|
|
|
Tetanus (DTaP, Tdap, Td): I have been informed that by not receiving this vaccine, my child may be at increased risk of |
|
|
|
|
developing tetanus if exposed to this disease. Serious symptoms and effects of this disease include: “locking” of the jaw, |
Initials___________ |
|
|
|
|
|
|
|
|
difficulty in swallowing and breathing, seizures (jerking and staring), painful tightening of muscles in the head and neck, |
Date____________ |
|
|
|
||
|
|
|
and death. |
|
|
|
|
|
|
|
|
|
Pertussis (Whooping Cough) (DTaP, Tdap): I have been informed that by not receiving this vaccine, my child may be at |
Initials___________ |
|
|
|
increased risk of developing pertussis (whooping cough) if exposed to this disease. Serious symptoms and effects of this |
|
|
|
|
|
|
|
|
|
disease include: severe coughing fits that can cause vomiting and exhaustion, pneumonia, seizures (jerking and staring), |
Date____________ |
|
|
|
||
|
|
|
brain damage, and death. |
|
|
|
|
|
|
|
|
|
Polio: I have been informed that by not receiving this vaccine, my child may be at increased risk of developing polio if |
Initials___________ |
|
|
|
exposed to this disease. Serious symptoms and effects of this disease include: paralysis (can’t move parts of the body), |
|
|
|
|
|
|
|
|
|
meningitis (infection of the brain and spinal cord covering), permanent disability, and death. |
Date____________ |
|
|
|
||
|
|
|
|
|
|
|
|
Measles, Mumps, Rubella (MMR): I have been informed that by not receiving this vaccine, my child may be at increased |
|
|
|
|
|
|
|
|
|
risk of developing measles, mumps, and/or rubella if exposed to these diseases. Serious symptoms and effects of |
|
|
|
|
measles include: pneumonia, seizures (jerking and staring), brain damage, and death. Serious symptoms and effects of |
Initials___________ |
|
|
|
||
|
|
|
mumps include: meningitis (infection of the brain and spinal cord covering), painful swelling of the testicles or ovaries, |
Date____________ |
|
|
|
sterility, deafness, and death. Serious symptoms and effects of rubella include: rash, arthritis, and muscle or joint pain. If a |
|
|
|
|
|
|
|
|
|
woman gets rubella while she is pregnant, she could have a miscarriage or her baby could be born with serious birth |
|
|
|
|
defects such as deafness, heart problems, and brain damage. |
|
|
|
|
Haemophilus Influenza type b (Hib): I have been informed that by not receiving this vaccine, my child may be at |
|
|
|
|
|
|
|
|
|
increased risk of developing Hib if exposed to this disease. Serious symptoms and effects of this disease include: |
Initials___________ |
|
|
|
meningitis (infection of the brain and spinal cord covering), pneumonia, severe swelling in the throat that makes it hard to |
Date____________ |
|
|
|
||
|
|
|
|
|
|
|
|
breathe, infections of the blood, joints, bones, and covering of the heart, and death. |
|
|
|
|
|
|
|
|
|
Hepatitis B: I have been informed that by not receiving this vaccine, my child may be at increased risk of developing |
Initials___________ |
|
|
|
hepatitis B if exposed to this disease. Serious symptoms and effects of this disease include: jaundice (yellow skin or |
|
|
|
|
|
|
|
|
|
eyes), |
Date____________ |
|
|
|
||
|
|
|
|
|
|
|
|
Hepatitis A: I have been informed that by not receiving this vaccine, my child may be at increased risk of developing |
Initials___________ |
|
|
|
hepatitis A if exposed to this disease. Serious symptoms and effects of this disease include: jaundice (yellow skin or |
|
|
|
|
|
|
|
|
|
eyes), |
Date____________ |
|
|
|
||
|
|
|
|
|
|
|
|
Varicella (Chickenpox): I have been informed that by not receiving this vaccine, my child may be at increased risk of |
Initials___________ |
|
|
|
developing varicella (chickenpox) if exposed to this disease. Serious symptoms and effects of this disease include: severe |
|
|
|
|
|
|
|
|
|
skin infections, pneumonia, brain damage, and death. |
Date____________ |
|
|
|
Due to my religious beliefs, I request an exemption for my child from the required vaccine doses selected above. I am aware that if I change my mind in the future, I can rescind this exemption and obtain immunizations for my child.
Initials_________________________
I am aware that additional information about vaccine preventable diseases, vaccines and reduced or no cost vaccination services is available from my local county health department and Arizona Department of Health Services (www.azdhs.gov/phs/immun/).
I am aware that in the event the state or county health department declares an outbreak of a
Child’s Name ______________________________________________________ Date of Birth (month/day/year)__________________________
Parent/Guardian Signature____________________________________________ Date (month/day/year)_________________________________
ADHS Immunization Program Office |
http://www.azdhs.gov/phs/immunization/ |
July 1, 2013 (rev: 9/1/18) |
Form Breakdown
| Fact Name | Details |
|---|---|
| Governing Law | The Arizona Religious Beliefs Exemption Form is governed by Arizona Revised Statutes § 15-873. |
| Purpose | This form is used by parents to document a religious exemption to immunizations for their children attending preschools and child care facilities. |
| Support for Immunization | The Arizona Department of Health Services (ADHS) emphasizes the importance of immunization as a key tool in preventing serious diseases. |
| Parental Rights | ADHS respects the rights of parents who choose not to vaccinate their children based on their religious beliefs. |
| Potential Risks | The form outlines the potential health risks associated with not vaccinating, including severe illnesses and complications from various diseases. |
| Rescinding Exemption | Parents can rescind the exemption at any time and choose to have their children vaccinated in the future. |