Fill Out Your Care 1St Arizona Prior Authorization Form
The Care 1St Arizona Prior Authorization form is an essential document for individuals seeking healthcare coverage, particularly for those with disabilities who are between the ages of 16 and 65. This form is designed to collect vital information about the applicant, including personal details such as name, address, and contact information. It also requires information about employment, income, and any existing health insurance coverage. Applicants must indicate their preferred language for communication and can request interpreter services at no cost if needed. The form emphasizes the importance of providing accurate information and outlines the rights and responsibilities of the applicant, including the need to report any changes in circumstances. Additionally, it includes sections for detailing assets and resources, as well as previous applications for Social Security Disability or Supplemental Security Income. By completing this form, applicants take a significant step towards accessing the medical benefits they may qualify for, ensuring they receive the necessary support for their healthcare needs.
Guide to Writing Care 1St Arizona Prior Authorization
Completing the Care 1St Arizona Prior Authorization form is a crucial step in securing healthcare coverage for individuals with disabilities. This process requires careful attention to detail, ensuring that all necessary information is accurately provided. Once the form is filled out, it will be submitted for review, which can lead to the approval of essential health services.
- Gather necessary information: Collect all relevant documents, such as proof of income, health insurance details, and personal identification, to ensure you have everything needed to complete the form.
- Fill out your personal information: Start with your name, home address, mailing address, and phone numbers. Be sure to provide accurate details to avoid delays.
- Provide information about yourself and your spouse: Include your Social Security number, date of birth, sex, race, and citizenship status. If your spouse is not applying, you do not need to provide their Social Security number.
- Detail your employment: List all jobs or businesses you have, including employer names, addresses, phone numbers, and your gross income. If self-employed, include details about your business and attach relevant tax documents.
- Report additional income: Indicate whether you receive any other types of income, such as Social Security or retirement benefits. Provide sources and amounts, and include proof where necessary.
- Disclose health insurance information: If you have Medicare or other health insurance, provide the insurance company name, policy number, and monthly costs. Attach proof of coverage and premium payments.
- List your assets: If you have any assets, such as bank accounts or property, provide details including the value and any amounts owed. Attach proof of ownership and value.
- Indicate disability status: Answer questions about your disability and provide information about your medical providers, including their names and contact details.
- State how you learned about the Medicaid Purchase Plan: This information may help the agency improve outreach efforts.
- Sign and date the form: Ensure that you sign the form, confirming that all information provided is accurate. If applicable, have an agency representative sign as well.
After completing these steps, review the form for accuracy and completeness. Once satisfied, submit the form as instructed, and keep a copy for your records. This will help ensure that your application is processed smoothly and efficiently.
Browse Popular Forms
Establishing Paternity in Arizona - The document must include signatures of both parents, which need to be original on all copies submitted.
Arizona Form 285 - The IRS identification number for corporations can be included.
Common Questions
What is the purpose of the Care 1St Arizona Prior Authorization form?
The Care 1St Arizona Prior Authorization form is designed to help individuals with disabilities who are between the ages of 16 and 64 apply for healthcare coverage. It is specifically tailored for those who are working and need assistance in accessing Medicaid services. By completing this form, applicants can provide necessary information about their personal circumstances, income, and medical needs, which will be used to determine their eligibility for coverage.
How can I get assistance in filling out the form?
If you find yourself needing help with the Care 1St Arizona Prior Authorization form, you have options. You can call your local Medicaid office for guidance. Additionally, there is a toll-free number, 1-888-544-7996, where you can speak with someone who can assist you. For individuals who are deaf or have hearing issues, a TTY line is available at 1-800-220-5404. Interpreter services are also offered at no cost, ensuring that language barriers do not prevent you from accessing the help you need.
What information do I need to provide about my income?
Do I need to provide information about my medical providers?
Yes, the form requires you to provide information about your medical providers. This includes the names and contact details of the doctors or healthcare professionals who care for you. This information is essential for the review process, as it helps Medicaid understand your healthcare needs and how they relate to your application for coverage.
What should I do if my situation changes after submitting the form?
If there are any changes in your circumstances after you have submitted the Care 1St Arizona Prior Authorization form, it is crucial to inform Medicaid within 10 days. Changes that need to be reported include moving out of state, alterations in your living situation, changes in your health insurance coverage, or shifts in your employment status. Keeping Medicaid updated ensures that your coverage remains accurate and that you continue to receive the benefits for which you are eligible.
Dos and Don'ts
When filling out the Care 1St Arizona Prior Authorization form, there are important steps to follow to ensure your application is processed smoothly. Here’s a list of things you should and shouldn’t do:
- Do: Fill out every item on the form completely. Missing information can delay your application.
- Do: Provide accurate details about your income and assets. This includes sending any necessary proof, like pay stubs or tax forms.
- Do: Use “none” if an answer to a question is zero or not applicable. This clarifies your response.
- Do: Contact your local Medicaid office or the provided toll-free number if you need assistance while completing the form.
- Don’t: Leave any sections blank. Each item is crucial for determining your eligibility.
- Don’t: Provide false information or omit details. This can lead to legal consequences and may affect your eligibility for benefits.
By following these guidelines, you can help ensure that your application for healthcare coverage is handled efficiently and accurately.
Similar forms
The Care 1St Arizona Prior Authorization form shares similarities with the Medicaid Application form. Both documents require detailed personal information, including the applicant's name, address, and contact details. They also inquire about household income and assets, ensuring that applicants meet the necessary financial criteria for eligibility. Additionally, both forms emphasize the importance of providing accurate information and the consequences of failing to do so, highlighting the legal obligations associated with Medicaid applications.
Another document that resembles the Care 1St Arizona Prior Authorization form is the Supplemental Nutrition Assistance Program (SNAP) application. Like the prior authorization form, the SNAP application collects personal information, income details, and household composition. It aims to determine eligibility for food assistance programs. Both forms also provide options for language assistance and emphasize the need for applicants to report any changes in their circumstances promptly.
The Social Security Disability Insurance (SSDI) application is another document with similar characteristics. Both forms require individuals to provide personal identification, income information, and medical history. They serve to establish eligibility for benefits based on disability status. Furthermore, both documents include a declaration of truthfulness, where applicants must affirm that the information provided is accurate and complete.
The Medicare application form also shares key features with the Care 1St Arizona Prior Authorization form. Both documents require personal and financial information to assess eligibility for health coverage. They ask about existing health insurance and require proof of income and assets. Additionally, both forms provide guidance on what to do if applicants need assistance completing them, ensuring accessibility for all users.
The Veterans Affairs (VA) health care application form is another comparable document. Similar to the Care 1St Arizona Prior Authorization form, it collects personal information and details about the applicant's military service. Both forms assess eligibility for health benefits and require applicants to disclose income and asset information. The VA form also emphasizes the importance of providing accurate information and the potential consequences of misrepresentation.
The Children's Health Insurance Program (CHIP) application is akin to the Care 1St Arizona Prior Authorization form in that both target specific populations needing health coverage. They require personal information about the child and their family, including income and household size. Both documents also highlight the importance of reporting changes in circumstances and provide options for assistance in filling out the forms.
The Temporary Assistance for Needy Families (TANF) application shares similarities with the Care 1St Arizona Prior Authorization form as well. Both require detailed information about the applicant's household, income, and expenses to determine eligibility for financial assistance. They also stress the need for accurate reporting and provide resources for applicants who may need help completing the forms.
The Federal Employee Health Benefits (FEHB) enrollment form is another document that resembles the Care 1St Arizona Prior Authorization form. Both forms require personal information and details about existing health coverage. They assess eligibility for health benefits and include sections for reporting income and dependents. Both documents also inform applicants about their rights and responsibilities regarding the information provided.
The Affordable Care Act (ACA) Marketplace application is similar to the Care 1St Arizona Prior Authorization form in that both aim to determine eligibility for health insurance coverage. They require personal and financial information, including household income and family size. Both forms emphasize the importance of providing accurate information and outline the consequences of failing to do so, ensuring that applicants understand their responsibilities.
Lastly, the Long-Term Care Insurance application shares characteristics with the Care 1St Arizona Prior Authorization form. Both documents gather detailed personal information, including medical history and financial details, to assess eligibility for benefits. They also require applicants to disclose any existing insurance coverage and provide documentation to support their claims. Both forms highlight the importance of accuracy and completeness in the application process.
Key takeaways
Filling out the Care 1St Arizona Prior Authorization form requires attention to detail and accuracy. Here are some key takeaways to consider:
- Complete Every Section: Ensure that all sections of the form are filled out completely. If a question does not apply, write “none” or “0” to indicate that.
- Provide Accurate Information: Double-check all personal information, including names, addresses, and Social Security numbers. Inaccurate information can delay the processing of your application.
- Include Proof of Income: Attach copies of recent pay stubs or other proof of income as required. This documentation is essential for verifying your financial situation.
- Use Available Resources: If you need assistance with filling out the form, do not hesitate to contact your local Medicaid office or call the provided toll-free numbers for help.
- Understand Your Rights: Familiarize yourself with your rights and responsibilities as outlined in the form. This includes the obligation to report any changes in your situation within ten days.
By following these guidelines, applicants can improve their chances of a smooth application process for healthcare coverage through the Medicaid Purchase Plan.
Common mistakes
-
Incomplete Information: One of the most common mistakes is not filling out every item on the form. Each section must be completed. If a question does not apply, write “none” instead of leaving it blank.
-
Missing Documentation: Applicants often forget to include necessary documents, such as pay stubs or proof of income. Providing this documentation is essential for verifying the information provided on the form.
-
Incorrect Income Reporting: Many people mistakenly report their take-home pay instead of their gross income. It is crucial to show the total income before any deductions.
-
Ignoring the Language Preference Section: Some applicants overlook the section asking about language preferences. This information helps ensure that applicants receive the appropriate support and services.
-
Not Providing Spouse Information: If the applicant is married, they may neglect to include their spouse’s information, even if the spouse is not applying. This can lead to delays or complications in processing the application.
-
Failure to Report Other Insurance: Applicants sometimes forget to mention any existing health insurance coverage. This is important as it affects eligibility and the processing of the application.
-
Missing Signature: A signature is required at the end of the application. Without it, the application cannot be processed, and it will be returned.
-
Not Following Up: After submitting the form, many applicants do not follow up to check the status of their application. Staying informed can help address any issues that may arise during processing.
Document Preview
BHSF Form
Rev. 04/05
Prior Issue Obsolete
II
For Agency Use Only
Request date |
|
(Application date) |
Date mailed
Agency Rep
To protect your application date, we must receive this application by |
|
. |
(for agency use only)
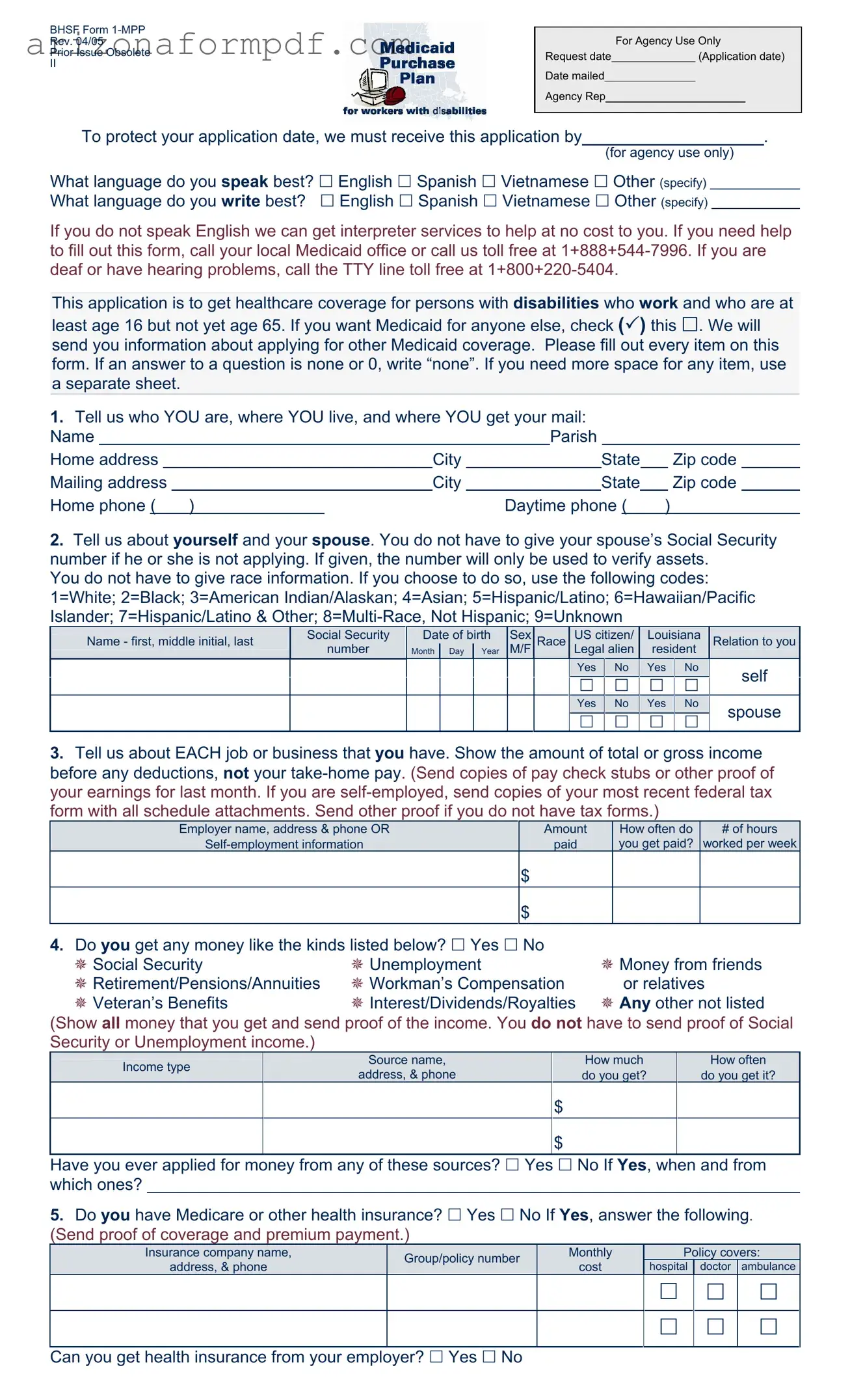
What language do you speak best? English Spanish Vietnamese Other (specify) What language do you write best? English Spanish Vietnamese Other (specify)
If you do not speak English we can get interpreter services to help at no cost to you. If you need help to fill out this form, call your local Medicaid office or call us toll free at
This application is to get healthcare coverage for persons with disabilities who work and who are at
least age 16 but not yet age 65. If you want Medicaid for anyone else, check ( ) this . We will send you information about applying for other Medicaid coverage. Please fill out every item on this form. If an answer to a question is none or 0, write “none”. If you need more space for any item, use a separate sheet.
1.Tell us who YOU are, where YOU live, and where YOU get your mail:
Name |
|
|
|
Parish |
|
|
|
|
||||||
Home address |
|
City |
|
|
State |
|
Zip code |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Mailing address |
|
City |
|
|
State |
|
Zip code |
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|||
Home phone ( ) |
|
Daytime phone ( |
) |
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
2.Tell us about yourself and your spouse. You do not have to give your spouse’s Social Security number if he or she is not applying. If given, the number will only be used to verify assets.
You do not have to give race information. If you choose to do so, use the following codes: 1=White; 2=Black; 3=American Indian/Alaskan; 4=Asian; 5=Hispanic/Latino; 6=Hawaiian/Pacific Islander; 7=Hispanic/Latino & Other;
Name - first, middle initial, last |
Social Security |
Date of birth |
Sex |
Race |
US citizen/ |
Louisiana |
Relation to you |
||
|
number |
Month |
Day |
Year |
M/F |
|
Legal alien |
resident |
|
|
Yes |
|
No |
|
Yes |
|
No |
|
self |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|||||||
|
Yes |
|
No |
|
Yes |
|
No |
|
spouse |
|
|
|
|
|
|
||||
3.Tell us about EACH job or business that you have. Show the amount of total or gross income before any deductions, not your
Employer name, address & phone OR |
Amount |
How often do |
# of hours |
paid |
you get paid? |
worked per week |
$
$
4.Do you get any money like the kinds listed below? Yes No
Social Security |
Unemployment |
Money from friends |
Retirement/Pensions/Annuities |
Workman’s Compensation |
or relatives |
Veteran’s Benefits |
Interest/Dividends/Royalties |
Any other not listed |
(Show all money that you get and send proof of the income. You do not have to send proof of Social Security or Unemployment income.)
|
Income type |
|
Source name, |
|
|
How much |
|
How often |
|
|
|
address, & phone |
|
|
do you get? |
|
do you get it? |
|
|
|
|
|
|
|
|
|
|||
|
|
|
|
|
$ |
|
|
|
|
$
Have you ever applied for money from any of these sources? Yes No If Yes, when and from which ones?
5.Do you have Medicare or other health insurance? Yes No If Yes, answer the following. (Send proof of coverage and premium payment.)
Insurance company name, |
Group/policy number |
Monthly |
|
Policy covers: |
|||
address, & phone |
cost |
hospital |
doctor |
ambulance |
|||
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Can you get health insurance from your employer? Yes No
6.Do you, or you jointly with your spouse, have any assets or resources like those listed below? Yes No If Yes, give us the following information. (Send proof of ownership and value.)
|
Asset/Resource |
Company name, address, & phone; |
Value |
Amount owed |
|
||||
|
Account number and/or description |
|||
|
|
|
|
|
|
Checking/Savings accounts (type) |
|
$ |
|
|
|
|
|
|
|
Certificates of Deposit |
|
$ |
|
|
Retirement accounts |
|
$ |
|
|
Annuities/Trusts |
|
$ |
|
|
Stocks/Bonds |
|
$ |
|
|
Vehicles (if more than one) |
|
$ |
$ |
|
Property, other than your home |
|
$ |
$ |
|
Other (please be specific) |
|
$ |
$ |
7.Did you ever apply for or get Social Security Disability or Supplemental Security Income (SSI)
benefits? Yes No If Yes, when? |
|
Was a decision made? Yes No |
|
If Yes, what was the decision? |
|
|
|
|
|
|
|
8.What is your disability?
Tell us about the doctors or other medical providers who care for you:
Provider’s name(s)
Address & phone of this medical provider
9.Where did you find out about the Medicaid Purchase Plan?
Rights and Responsibilities
I declare that I am a U.S. citizen or in this country legally.
The information I gave on this form is true and correct to the best of my knowledge. I realize if I knowingly give information that is not true OR if I knowingly hold back information, I may get health benefits for which I am not eligible. If that happens, I can be lawfully punished for fraud. I may also have to pay Medicaid back for any medical bills which are paid incorrectly.
I understand that the information I give about my situation will be checked. I agree to help do that, and to let Medicaid get information it needs from government agencies, employers, medical providers, and other sources. If I refuse to help with this process or in later reviews caused by reported changes, or as part of a Recipient Eligibility review, it will mean that I can’t get Medicaid until I do help.
I know that Social Security numbers will only be used to get information from other government agencies to prove my eligibility.
I agree to tell Medicaid within 10 days if 1) I move out of state; 2) there are changes in where I live or get my mail; 3) there are any changes in other health insurance coverage; 4) there is any change in my work status.
By accepting Medicaid, I agree that any medical payments received from other sources will be sent to the Department of Health and Hospitals for any services that were covered by Medicaid.
I can ask for a Fair Hearing if I think the decision made on my case is unfair, incorrect or being made too late.
Medicaid can’t treat me differently because of my race, color, sex, age, disability, religion, nationality or political belief. If I think they have, I can call the U.S. DHHS Regional Office for Civil Rights in Dallas, TX at
Signature of Applicant or Authorized Representative |
|
Date |
|
|
|
Signature of Agency Representative, if applicable |
|
Date |
Form Breakdown
| Fact Name | Description |
|---|---|
| Application Purpose | This form is used to apply for healthcare coverage under Medicaid for individuals with disabilities who are between the ages of 16 and 64. |
| Language Assistance | If you do not speak English, interpreter services are available at no cost to help you fill out the form. |
| Income Reporting | Applicants must report total or gross income from all jobs or businesses before any deductions. Proof of income is required. |
| Assets Disclosure | Applicants must disclose any assets or resources they own, including bank accounts, vehicles, and property. Documentation of ownership and value is needed. |
| Legal Compliance | Providing false information can lead to penalties, including being required to repay Medicaid for any incorrectly paid medical bills. |